
Hair loss treatment in Saarbrücken
The satisfaction of our patients is underlined by the results of scientific publications. Is your hair thinning or are you already suffering from hair loss? Does no caffeine shampoo give you the desired result? Do you want to have thicker and fuller hair again?
Opt for more hair and more satisfaction:
- Fuller and thicker hair
- Pleasing yourself from all angles
- wear the hairstyle you want
- Professional advice
What our patients say
Information at a glance

Duration of treatment
30 minutes

Anesthesia
Anesthetic cream / vibration anesthesia

Hospitalization
Outpatient

Socially acceptable
after 2 weeks

Costs

Additions or alternatives

Does a treatment with processed own blood help against hair loss?
Treatment with your own blood stops hair loss and stimulates hair growth. There are numerous scientific studies that prove the benefits of the treatment [21] [22] [23] [24]. The treatment should usually be repeated three times. The effect of the patient’s own blood has been used successfully for many years to support hair transplants [25].
Platelets contain numerous growth factors and stimulating mediators. Growth factors such as insulin-like growth factor (IGF-1), hepatocyte growth factor (HGF), keratinocyte growth factor and vascular endothelial growth factor (VEGF) promote the growth phase of the hair cycle [26]. The positive effect of many of these growth factors on hair growth has been scientifically proven [27].
Does microneedling help against hair loss?
Microneedling is a safe procedure for the treatment of acne scars, mouth wrinkles, crow’s feet, burn scars and pregnancy marks, either alone or in combination with other procedures [28]. Studies have shown that hair density and hair thickness increase faster and more strongly with the combination treatment with the patient’s own blood and microneedling than with treatment with the patient’s own blood alone [29] or with microneedling treatment alone [30]. Microneedling is a minimally invasive procedure in which several fine needles are used to create micropunctures in the skin. The treatment takes about 30 to 45 minutes and is repeated three to six times at intervals of two to four weeks.
Structure of a hair and a hair organ
The follicle (hair follicle) is the cell structure in which a hair develops and grows. Follicles extend from the hair funnel to the hair root. In the center of the follicle lies the hair, which is covered by the hair root sheath. The base of the follicle, also known as the hair bulb or bulbus, lies four millimeters below the surface of the skin. The horn cells of the hair emerge from the stem cells of the hair bulb. In addition, the stem cells of a hair follicle support wound healing. Each hair follicle is connected to a hair erector muscle, a sebaceous gland and often also a sweat gland [6] . Hair can grow individually or in groups of two to three or even four to five hair follicles.
The hair shaft consists of three layers: an outer cuticle layer (cuticle), the outer cortex layer (cortex) and the medulla. The hair fiber consists of dead horny cells, the so-called keratinocytes. These specialized cells produce the protein keratin and absorb color pigments from the skin’s pigment cells [7] .
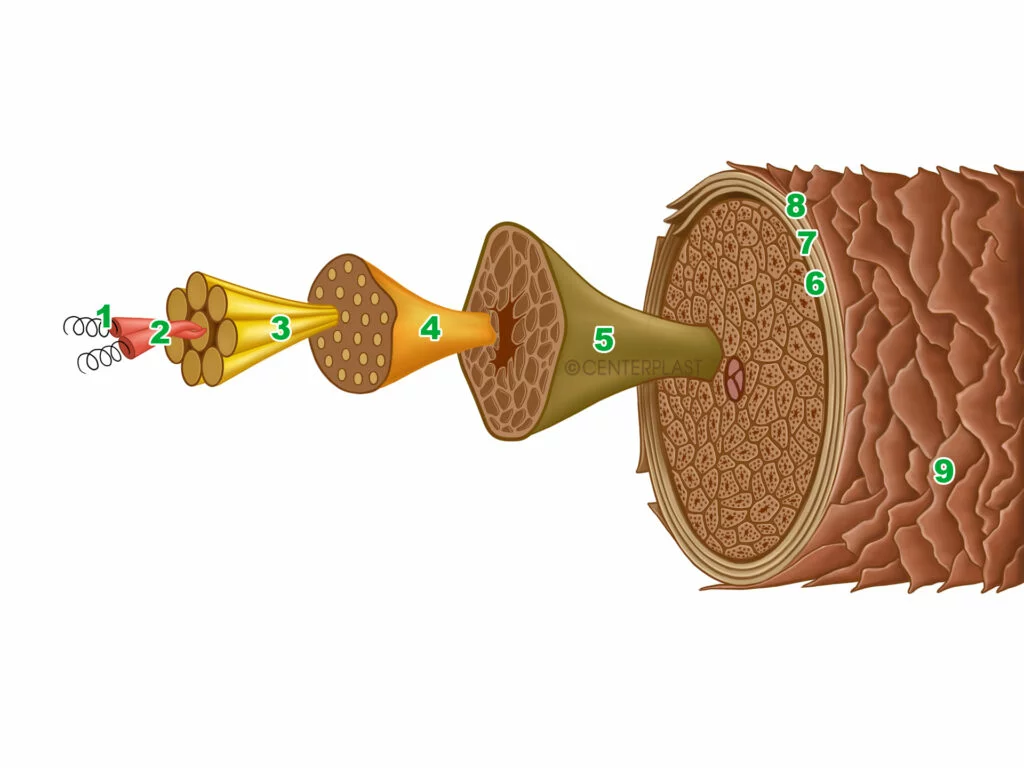
Schematic Cross Section Hair Fiber
The composition and complex structure of the hair determine its properties. Depending on humidity, hair consists of 65 to 95 percent keratin and up to 32 percent water. A small percentage of hair also consists of fats [8] . The spiral-shaped α-keratin is also an important component of the skin and nails. Four keratin chains together form a protofilament. Eight protofilaments in turn form an intermediate filament. These bundle together to form macrofibrils, which unite to form cortex cells. Several cortex cells, surrounded by an outer cuticle layer, form a hair shaft. Each scale has an average length of 60 micrometers and a thickness of about 0.5 micrometers [9] .
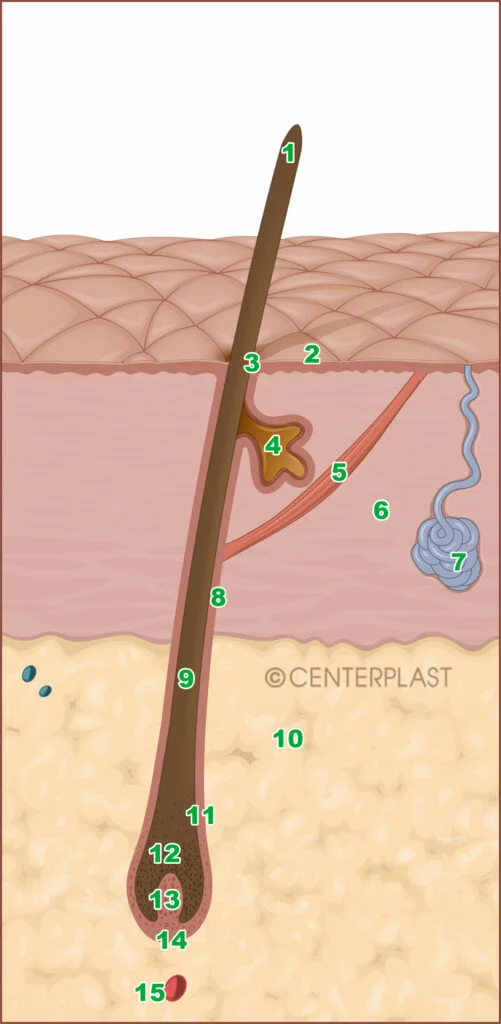
Cross section skin
Hair loss due to environmental pollutants
Pollutants and environmental toxins are becoming increasingly common. Pollutants can be absorbed in very different concentrations through the air we breathe or through food. Sudden (acute) poisoning is usually accompanied by severe, sometimes life-threatening symptoms shortly after ingesting a large quantity of harmful substances. Chronic poisoning (long-term poisoning) is often difficult to diagnose. Nonspecific and mild symptoms long after the onset of poison intake over a long period of time make suspicion difficult. In very rare cases, hair loss can be a sign of chronic poisoning. In justified cases of suspicion, traces can be detected in the blood, urine or hair, depending on the poison.
- Pollutant sources in the environment with mercury: coal-fired power plants, gold washing, smelting furnaces, cement production. Use in batteries, lamps or thermometers is no longer permitted.
- Pollutant sources with mercury for humans: Dental amalgam, contaminated fish, exposure to pollutants in the workplace. An amalgam dental filling releases 2 to 28 micrograms of mercury per day [10].
- Mercury limits: According to the WHO, two micrograms of mercury per kilogram of body weight per day (IPCS (2003) Concise International Chemical Assessment Document, World Health Organization).
- Signs of mercury poisoning: fatigue, depression, insomnia, irritability, memory loss, hair loss [11] .
- Sources of pollutants in the environment Cadmium: alloys, paints, solder.
- Sources of cadmium harmful to humans: Cigarette smoke, use of contaminated fertilizers, shellfish, crustaceans, offal, sunflower seeds, peanuts and linseed [12] .
- Cadmium limits: According to the European Food Safety Authority, the tolerable weekly intake of cadmium is 2.5 micrograms per kilogram of body weight.
- Signs of cadmium poisoning: Cadmium damages the kidneys, bones, blood formation, hormone balance and can lead to hair loss [13]. Cadmium accumulates in the liver and kidneys over decades.
- Pollutant sources of arsenic in the environment: combustion of fossil fuels, lead alloys, light-emitting diodes, pest control, wood preservatives, glass production.
- Sources of arsenic for humans: contaminated grain, rice, beer and drinking water.
- Arsenic limits: The European Food Safety Authority has set a health risk limit of 0.3 to 8 micrograms per kilogram of body weight per day (Data Collection Reports – EFSA – 2015).
- Signs of arsenic poisoning : Acute poisoning is accompanied by fatigue, nausea, vomiting and diarrhea. Chronic arsenic poisoning is characterized by weight loss, hair loss on the scalp, eyebrows and eyelashes, thickening of the phalanges of the fingers and enlargement of the nail bed.
- Pollutant sources of thallium in the environment: pest control against rodents, ants and cockroaches, production of semiconductors and alloys.
- Limit values for thallium: The U.S. Environmental Protection Agency assumes a harmful limit value of 0.01 milligrams per kilogram of body weight per day.
- Signs of thallium poisoning: It is tasteless, odorless and colorless. In small amounts, thallium leads to hair loss; larger amounts cause sensory disturbances, diarrhea, nausea and vomiting. Hair loss sets in two to three weeks after thallium poisoning [44]. Eyebrow hair loss is frequently observed [45].
- The trace element selenium is an important component of many proteins in the body, especially enzymes of the thyroid hormone metabolism, enzymes for defense against free radicals and white blood cells.
- Pollutant sources of selenium for humans: Sea salt, offal, yeast, bread, mushrooms, asparagus, rapeseed, broccoli, cabbage, garlic, onions and leeks [46]. As selenium is enriched in animal feed, eggs and dairy products can also contain high levels of selenium. Brazil nuts are particularly high in selenium – up to 400 micrograms of selenium depending on the region where they are grown [47]. Certain anti-dandruff hair shampoos also contain selenium. Poisoning is also caused by overdosing food supplements with selenium [48].
- Selenium limits: For infants, an intake of 15 micrograms of selenium per day and for adults 70 micrograms per day is recommended. The Federal Institute for Risk Assessment recommends a maximum limit of 300 micrograms per day. Signs of poisoning: palpitations, chills, concentration problems, gastrointestinal complaints, hair loss and nail growth disorders.
No two hairs are alike
Scalp hair is as diverse as the human being. That’s why our hair is often an expression of our personality. Hair is a part of our body and its condition reflects our overall health. Hair plays an important role in thermoregulation, the sense of touch, protection against ultraviolet (UV) radiation from the sun and wound healing. In addition to the length or color of the hair, hair can have many different characteristics:
- Hair texture: The shape of the hair can be divided into categories: completely straight, almost straight, wavy, large curls, Afro curls, very small Afro curls. Curly or straight hair is usually hereditary. In rare cases, curls can be a side effect of certain medications (retinoids) [10].
- Number of hairs: blondes have an average of 140,000 hairs, dark-haired people 105,000 and redheads 90,000 hairs [11] .
- The density of the hair is measured in hair fibers per square centimeter. The density is about 170 hairs per square centimeter for Americans of Hispanic descent, 155 hairs per square centimeter for people of African descent, and 220 hairs per square centimeter for Europeans [12].
- Hair thickness: The diameter of a hair is around 65 micrometers for Europeans, 90 micrometers for Asians and 75 micrometers for Africans [13] .
- Shape of the cross-section: The cross-section of a hair is oval for European and African hair and round for Asian hair [14] .
- Surface roughness: The roughness of a hair is measured, among other things, as the difference in height between a peak and a valley on the surface of the hair. For European and African hair, the difference in height is 12 nanometers, for Asian hair 10 nanometers [15].
- Tensile strength: Scientists speak of the tensile strength of hair. On average, a hair can withstand a maximum tension of 80 grams per millimeter before it breaks.
- Elasticity describes the extent to which a hair can return to its original shape after stress. A hair can be stretched by 20 to 30 percent of its length (modulus of elasticity 4.2 gigapascals) [16].
- Hair growth: In the scalp, each hair grows evenly, around 0.3 millimeters per day or one centimeter per month continuously over two to seven years.
- Hair loss: The proportion of growing hair compared to shedding hair is called the anagen-telogen ratio. In healthy young people, around 90 percent of hair is in the growth phase (anagen phase) and five to ten percent in the resting phase (telogen phase).
- Vellus hair (downy hair): Vellus hairs are hairs with a diameter of less than 30 micrometers. The proportion of vellus hair varies by 15 percent depending on age, gender, ethnic origin and scalp region [17].


Light hair and receding hairline
Alopecia is the technical term for reduced hair density, colloquially known as hair loss. The word “alopecia” comes from the ancient Greek word for “fox” άλώπηξ (alōpēx). The change of hair or a disease-related loss of hair in foxes may explain the origin of the word. Age-related changes in hair begin to appear as early as the age of 30 [18]. With age, hair becomes thinner, the density of the hair decreases, the pigments in the hair diminish and the scalp and hair become drier.
The first gray hairs appear on average from the age of 35 in Europeans and from the age of 44 in Africans. Hormones influence the distribution, resistance and color of the hair. Hereditary hair loss is often played down by those who are not affected [19]. As hair is an expression of youthfulness, health and attractiveness, the changes have an impact on our self-image. A hereditary predisposition or illness can lead to reduced hair density (medical term: alopecia) and therefore thinning hair. The decisive factor here is the ratio of hair that grows back to the hair that falls out.
Light hair is often perceived as a psychological burden and can impair quality of life [20]. In fact, bald men are seen by women as older, less attractive, less successful in the workplace and in finding a partner [21]. It has been shown that both men and women with hormone-induced hair loss suffer more from anxiety and depression [22].

Causes of hair loss
Hereditary hair loss (androgenetic alopecia)
This is the most common form of hair loss and is influenced by genes and hormones.
What are the causes of hereditary hair loss?
The activation of the hormone receptor shortens the growth phase of the hair cycle.
Spread of hereditary hair loss
Thirty percent of European men are affected by the age of 30, 50 percent by the age of 50 and 80 percent by the age of 70 [23]. Around 15 to 20 percent of European women between the ages of 30 and 50 suffer from this hereditary hormonal form of hair loss. Up to 30 percent of post-menopausal women suffer from androgenetic alopecia [24]. Asians and Africans are less frequently affected than Europeans.
Symptoms of hereditary hair loss
The hair becomes thinner and shorter and eventually barely penetrates the skin. In men, hair thinning occurs in the temple area, which spreads to the crown of the head over the years. In women, diffuse alopecia (diffuse hair loss) occurs on the crown of the head.
How can the diagnosis be made?
The diagnosis is made by visual inspection (clinical examination) of the hair and scalp. The pale patches and fine hair are characteristic, making it easier to recognize the most common cause. The ratio of normal hairs to downy hairs is less than 4:1 (normal value 7:1). An increase in hair loss (severe hair loss) is usually not observed when the hair is pulled through (Sabouraud maneuver) or during the hair pull test. If diffuse hair loss, brittle hair and nails are observed and increased tiredness is complained of, a blood test for thyroid hormones may be indicated. With magnification, downy hairs (vellus hairs) can be seen in the clear areas during the physical examination. A computer-assisted examination of the growth behavior (TrichoScan) or the examination of the epilated hair (trichogram) or excised hair roots (scalp biopsy) under the microscope are usually not necessary.
How can hereditary hair loss be treated?
Hereditary hair loss is usually treated with needling, a solution of the active ingredient minoxidil, processed autologous blood and finasteride tablets.
Is there anything I can do to prevent it?
Proper hair care, a balanced diet, avoidance of stress, normal body weight (BMI: between 18.5 and 24.9), no tobacco consumption.
Prognosis for hereditary hair loss:
The risk of hereditary increased hair loss is significantly increased if the father, mother or grandfather suffered from hair loss [25]. The speed of progression is unpredictable. Some men go completely bald in less than five years, but most take 15 to 25 years.
Circular hair loss (alopecia areata)
Cause of circular hair loss
Examinations indicate an autoimmune disease in which the body’s own white blood cells (T cells) attack the body’s own hair roots.
Distribution and occurrence
Circular hair loss occurs in 0.2 percent of the population, regardless of gender, age and ethnic origin. Around two percent of the general population suffers from this form of hair loss at some point in their lives [26]. Patients with white spot disease (vitiligo) or autoimmune thyroid disease are more frequently affected.
Symptoms of circular hair loss
The hair can fall out in batches in circumscribed areas all over the body. The scalp or beard is usually affected.
How can I find out if I have circular hair loss?
The diagnosis can be made on the basis of the pattern of hair loss. Occasionally, punctiform indentations or grooves form on the nails. The hair can be easily plucked from the edges of the hairless areas. Typical signs of circular hair loss can be recognized with magnifying glasses. The diameter of the hair shaft tapers near the hair follicle. Because of the altered shape, they are referred to as cob hairs or comma hairs. Black dots can be a sign that the hair has broken off directly at skin level. White hairs occasionally grow in the clear areas. Because of the characteristic appearance, a biopsy is rarely necessary.
How can circular hair loss be treated?
A cortisone injection (triamcinolone, five to ten milligrams per milliliter) every two to six weeks stimulates hair regrowth in 60 to 67 percent of cases [27]. Side effects of cortisone treatment include thinning of the skin, vascular markings and white patches [28]. Injecting the body’s own blood is a safe and effective method with success rates of up to 76 percent [29]. Comparative studies have confirmed the effectiveness and tolerability of the treatment method using the patient’s own blood [30].
Can I prevent circular hair loss?
As stress can trigger a bout of hair loss, a balanced lifestyle should be sought.
Prognosis for circular hair loss
After initial hair loss, the hair grows back on its own in 50 to 60 percent of cases. If there is a family history of circular hair loss, the episodes of hair loss often recur [31].
Diffuse hair loss (telogen effluvium)
Cause of diffuse hair loss
The hair follicles enter the resting phase (telogen phase) prematurely. In about a third of cases, no trigger can be found. The known triggers include: Medication such as the contraceptive pill (birth control pill), vitamin A (retinoids), blood pressure medication (beta blockers, ACE inhibitors), antidepressants and anticoagulants (heparin), hyper- or hypothyroidism, kidney or liver failure, childbirth, physical stress such as severe illness, inflammation, autoimmune diseases, surgery, a radical diet, emotional stress.
Distribution and frequency
Exact figures on the frequency of diffuse hair loss are not known. Both men and women are affected.
Symptoms of diffuse hair loss
Hair loss can occur suddenly or gradually. Hair loss usually occurs around two to three months after a triggering event. This leads to thinning of the hair and diffuse hair loss over the entire scalp. The loss is normally no more than 50 percent of the scalp hair.
Diagnosis
The diagnosis can be made on the basis of the characteristic symptoms and the examination findings. Gradual diffuse hair loss and hereditary hair loss can appear very similar. In contrast to diffuse hair loss, hereditary hair loss in women mainly affects the crown of the head and produces more downy hair. The ratio of normal hairs to downy hairs is greater than 8:1 (normally 7:1). In case of doubt, the diagnosis can be confirmed by taking a tissue sample from the scalp. Depending on the symptoms, further tests may be arranged, such as a blood test to determine thyroid levels, vitamin B12 and vitamin D3 levels, iron levels and zinc levels.
Treatment of diffuse hair loss
In the case of sudden diffuse hair loss, normal hair growth resumes once the trigger has been removed. If an autoimmune disease is the cause of chronic diffuse hair loss, a topical application of cortisone is advisable. The treatment is safe, well tolerated and can be helpful in cases of chronic diffuse hair loss. A minoxidil solution can be used in chronic cases [32].
Prevention of diffuse hair loss
The risk of diffuse hair loss is reduced by gentle hair care, a balanced diet and a healthy lifestyle.
Prognosis diffuse hair loss
If the diffuse hair loss starts suddenly and a trigger can be identified, it can be assumed that the hair will grow back completely.
Patterns of hair loss
Hormonal-hereditary hair loss (androgenetic alopecia) affects both men and women. As the name suggests, hair loss in this case is related to hormonal changes and genes. However, the regions of hair loss differ between the two sexes. In men, hair loss occurs on the temples and forehead, while in women the hair on the crown of the head thins out. Various classifications provide orientation about the pattern and severity of hair loss.
Simple classifications are often imprecise, while complex classifications also include transitional forms and gradations. However, complex classifications are less reliable. This means that when applying the same classification to the same case, different users may arrive at different classifications. Due to their user-friendliness, the Norwood-Hamilton classification is widely used for male pattern hair loss and the Ludwig classification for female pattern hair loss. Classifications are of practical use if a standardized treatment recommendation can be derived from the stage of hair loss. However, there is currently still a lack of scientific evidence for the benefits of a stage-appropriate treatment concept.
Male pattern hair loss (Hamilton-Norwood classification)
In 1951, James B. Hamilton categorized the hair loss of 300 men into eight stages [33]. The American physician O’Tar Norwood supplemented Hamilton’s classification in 1975 with rare patterns in which the hair loss on the temples and forehead progresses simultaneously [34]. In the classic hair loss pattern, the temples are affected first and later the crown of the head until the bald area covers the entire top of the skull and hair only remains at the back of the head. This pattern of hair loss can also rarely occur in women.
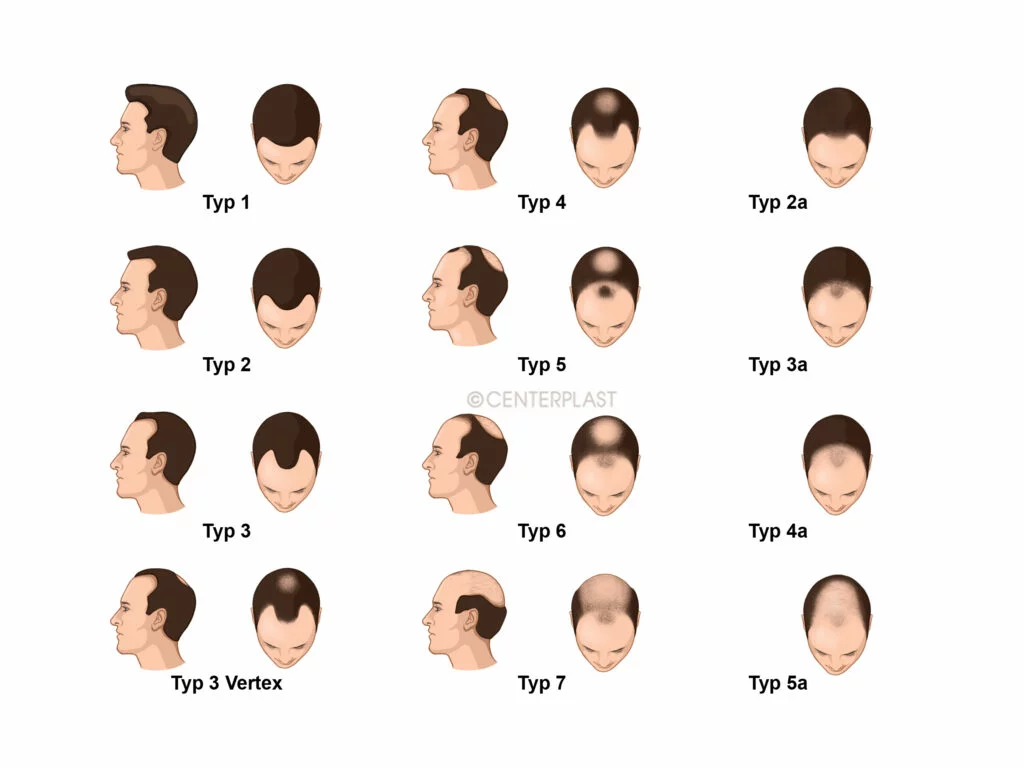
- Type 1: The hairline at the temples has receded minimally.
- Type 2: The hair thins above the temples. The so-called receding hairline develops.
- Type 3: Lateral depressions develop on the temples. In vertex type III vertex, a bald spot develops early on at the back of the head, also known as the crown of the head or tonsure (“plate”).
- Type 4: The indentations are pronounced. There are only a few hairs on the crown of the head. The hairy zone in the crown area is wider than in stage V.
- Type 5: The hairy zone at the crown of the head becomes thinner and the hair density has decreased further. The hairline of the temples and forehead has shifted further towards the back of the head.
- Type 6: The bald area spans the temporal regions and the crown of the head.
- Type 7: This is the most severe form of hair loss. All that remains is a narrow, horseshoe-shaped hair band on the sides and back of the scalp. The hair at the back of the head is also thin and the hair density is low.
Scheme of hair loss in women (Ludwig and Sinclair classification)
In women, hormonal-hereditary hair loss (androgenetic alopecia) leads to a reduction in the volume of hair on the top of the head. The thinning begins at the crown and spreads to all sides over time. As with men, the hair in the affected areas becomes thinner and shorter until downy hair (vellus hair) eventually develops. The pattern of hair loss in women was first divided into three stages by the doctor Erich Ludwig from Hamburg in 1977 [35].
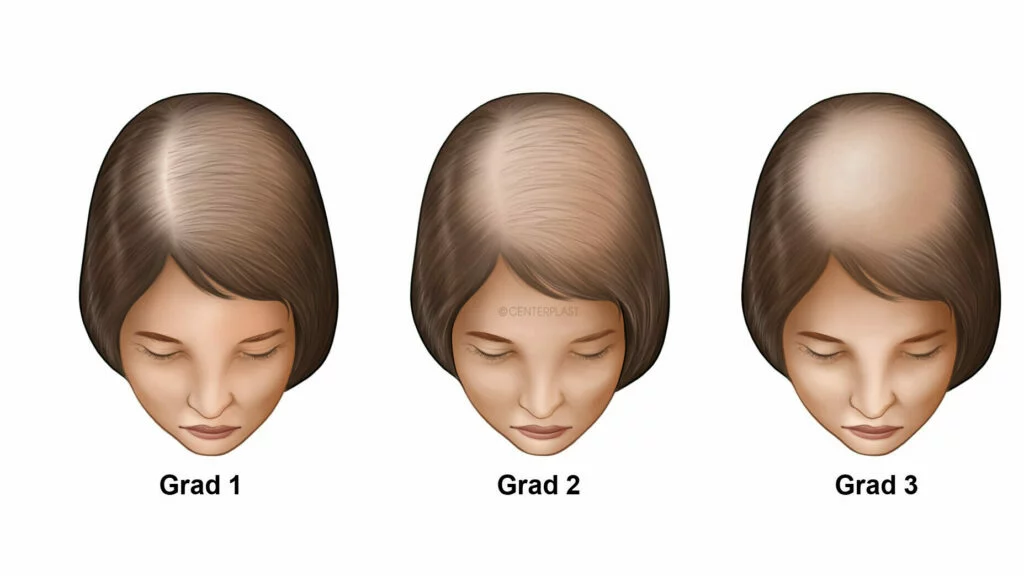
- Grade 1: The hair is thinner on the top of the head. The affected area is located one to three centimeters behind the hairline of the forehead.
- Grade 2: The hair density on the top of the head is significantly reduced and allows the scalp to shine through.
- Grade 3: In this most severe form, the top of the head is bald.
The Australian doctor Rodney Sinclair has divided the severity and pattern of hair loss into five stages [36] .

- Grade 1: Hair density and hair diameter in healthy women.
- Grade 2: The crown widens slightly.
- Grade 3: Beyond the parting, the hair lightens and becomes thinner.
- Grade 4: The density and diameter of the hair is reduced over the entire top of the head.
- Grade 5: The hair loss is very advanced and the scalp is clearly showing through
Care tips
What makes your hair look younger?
Thin hair:
Avoid long hairstyles. Long hair is straightened by its own weight. Perms can make the hair look thicker and give it more volume.
Gray hair:
Gray hair that has become thinner feels thicker with hair dye. Another technique is a step cut. With this technique, the hair on the top of the head is cut shorter than the hair on the bottom of the head. In women, this can give the appearance of long hair, although the upper part of the hair is quite short.
Brittle hair:
Use shampoos and conditioners that contain natural oils (coconut oil, olive oil, jojoba oil) to smooth the hair. Avoid damaging your hair with straightening treatments, hot tools and frequent coloring. Conditioners form a protective layer around the hair. However, broken hair or split ends cannot be repaired. Panthenol is absorbed into the hair shaft and has a moisturizing effect. Conditioners and shampoos can give hair more moisture and body [37].
Choosing the right shampoo
The cosmetics industry recommends a suitable shampoo for every need. A distinction must be made here as to whether the manufacturer promises an effect on the hair root or on the hair shaft. A shampoo that is supposed to stimulate hair growth with caffeine has an effect on the hair root. There is no independent scientific evidence that shampoos promote hair growth. Apart from the effectiveness of the active ingredients, it is doubtful that the substances can act in sufficient concentration and for a sufficiently long time when washing the hair. Nevertheless, high-quality shampoos can improve the hair’s resistance and the appearance of damaged hair by forming a protective layer [38].
A shampoo contains washing-active substances (surfactants), water, care substances and additives (preservatives, fragrances, colorants, thickeners). On average, a shampoo is made up of 10 to 30 ingredients [39]. The surfactants dissolve the fats in the water and form the foam. Washing-active substances are divided into four groups according to their water-binding charged content:
- Non-charged non-ionic surfactants
Representatives: Fatty alcohol alkoxylates, sorbitan esters, alkyl polyglucosides
Properties: Good cleaning properties, but poor foaming. - Negatively charged anionic surfactants
Representatives: Sodium lauryl sulphate, alkyl ether sulphates, alkyl ether carboxylates, sulphosuccinates, olefin sulphonates, vegetable soaps
Properties: Good cleansing power, produces a rich lather. - Positively charged cationic surfactants
Agents: Stearalkonium chloride, Behentrimonium methosulfate, Cetrimonium chloride
Properties: Have an antistatic effect, clean poorly and do not foam well. Therefore more likely to be used in hair conditioners and hair treatments. - Negatively and positively charged amphoteric surfactants (zwitterionic surfactants)
Representatives: Betaine, amphoteric acetate and diacetate
Properties: Good skin compatibility.
On average, three different surfactants are used in a shampoo. The most common are sodium lauryl ether sulfate, coconut betaine (cocamidopropyl betaine) and glycol distearate. So-called “baby shampoos” and normal shampoos do not differ in this respect [40].
Coconut betaine (cocamidopropyl betaine) is well tolerated by the skin and is made from coconut oil and dimethylaminopropylamine. Skin allergies that can occur with the external application of coco betaine are due to impurities with reaction intermediates (amidopropylamines) [41].
Shampoo ingredients that you should avoid
The detergent substances ammonium lauryl sulfate and sodium laureth sulfate are considered skin irritants and should be avoided [42] .
Certain additives in shampoos can trigger hypersensitivity reactions. These substances are also known as allergens. Particularly common allergens are the fragrances linalool, limonene, citronellol, hexyl cinnamaldehyde, benzyl salicylate and benzyl alcohol. The most common preservatives in shampoos include sodium benzoate, phenoxyethanol and benzoic acid. Interestingly, most “baby shampoos” and normal shampoos do not differ in terms of the preservatives used [43].
Additives from the ethanolamine group are used in shampoos to adjust the pH value. This group of substances includes monoethanolamines (MEA), diethanolamines (DEA) and triethanolamines (TEA). The substances can trigger allergies, skin irritation and asthma-like symptoms and are suspected of having a carcinogenic effect [44]. Minor but measurable side effects can be detected at concentrations hundreds of times higher than the use in cosmetics (Lim D.S., Roh T.H., Kim M.K., et al., 2018, J Toxicol Environ Health A.). Nevertheless, we recommend avoiding shampoos with MEA, DEA or TEA.
Phthalates are used in hair care products to make hair more supple. The representatives of this group include: Benzyl Butyl Phthalate (BBP), Diethylhexyl Phthalate (DEHP), Diethylhexyl Terephthalate (DEHTP), Dimethyl Phthalate (DMP), Di-Isobutyl Phthalate (DiBP), Di-n-Butyl Phthalate (DBP), Di-Isononyl Phthalate (DiNP). Phthalates are considered toxic to reproduction and can trigger allergies and asthma in children [45].
Bisphenols, in particular bisphenol A (BPA), are used in the production of plastics and can transfer from the packaging to the contents of the packaging [46]. Bisphenol A has hormone-like effects in the human body. Exposure to bisphenol A can impair fertility in men, disrupt thyroid function, cause high blood pressure, diabetes mellitus, obesity and breast cancer [47].
The sustainability of shampoos should also be a selection criterion, given the fact that the average European uses 2 kg of shampoo per year. In addition to the ingredients, packaging, production and transportation also have an impact on CO2 emissions and water pollution [48]. The washing-active substances (surfactants) in conventional shampoos are usually produced on a petroleum basis (ammonium lauryl sulphate and sodium lauryl sulphate). Plant-based soaps are more biodegradable.
Silicones make the hair smooth, supple and easier to comb. The silicones include dimethicone, dimethiconol, cyclomethicone, phenyltrimethicone, octamethylcyclotetrasiloxane (D4), decamethylcyclopentasiloxane (D5) and dodecamethylcyclohexasiloxane (D6) and amidomethicone. Silicones are persistent and can accumulate in the environment. Alternative ingredients are coco-caprylates, lauryl glucoside, coco glucoside, glyceryl oleate and PEG (polyethylene glycol) derivatives.
Hair Anti-Aging
Certain preparations, especially in combination, can counteract hereditary hair loss (androgenetic alopecia). Whether medication and which medication is suitable will be discussed with you during the examination. As with any treatment, the advantages and disadvantages must be carefully weighed up.
Minoxidil was patented in 1971 by the Upjohn company for the treatment of high blood pressure. What was initially a side effect led to approval by the US Food and Drug Administration in 1988 as a hair restorer for men and women over the age of 18.
Mechanism of action:
Minoxidil regulates the exchange of electrically charged particles of certain body cells (potassium channel blocker). As a result, the blood vessels dilate, allowing more oxygen and nutrients to reach the hair roots. The exact mechanism of action is still unclear. The solution contains alcohol and propylene glycol to increase the absorption of minoxidil into the tissue [49].
Application:
Minoxidil is available over the counter in two concentrations (two and five percent). Minoxidil is available as a solution (liquid form) or as a foam and should be applied in the morning and evening.
Side effects:
The most common adverse effects are a burning sensation, itching and scaling. The latter is mostly due to the alcohol and propylene glycol in the solution. Minoxidil causes a shortening of the resting phase (telogen phase) of the hair cycle. Temporary hair loss may therefore occur at the start of treatment. Allergic skin reactions to minoxidil or propylene glycol are possible. In the event of an allergic reaction to propylene glycol, the minoxidil foam can be used without propylene glycol.
A preparation was approved by the US Food and Drug Administration (FDA) in 1992 for the treatment of benign prostatic hyperplasia in a dosage of five milligrams. The occurrence of increased hair growth during treatment led to approval in 1998 for the treatment of hereditary hair loss (androgenetic alopecia) at a dosage of one milligram.
Mechanism of action:
The active substance (N-tert-butyl-3-oxo-4-aza-5α-androst-1-ene-17β-carbamide) inhibits an enzyme (5-alpha-reductase isoenzymes) of type II and III, which controls the conversion of testosterone into dihydrotestosterone (DHT). The type II enzyme is found in the hair root, the outer root sheaths of the hair follicles, the epididymis, the vas deferens, the seminal vesicles and the prostate gland [50]. The medication increases hair growth, particularly in the parting area. The maximum effect is achieved after one year.
Application:
The tablets are only available on prescription. A dosage of one milligram once a day is recommended for the treatment of hair loss. It can take four to six months before increased hair growth can be detected.
Side effects:
In the first few weeks, there may be a temporary increase in hair loss. The medication should not be used in women who wish to become pregnant, as it can affect the development of the sex in the event of pregnancy. The medication can reduce the desire for sexual intercourse and lead to erectile dysfunction. Depression has also been described. As a rule, these complaints decrease over time. Individual cases of persistent side effects after discontinuation of the tablets have been observed. The preparation also reduces the PSA value, a value used for the early detection of prostate cancer. There is therefore a risk that prostate cancer will be detected later if the tablets are taken.
Another drug has been approved by the American health authorities since 2001 and in Germany since 2003 for the treatment of benign prostate enlargement. The drug has only been approved for the treatment of hereditary hair loss in South Korea and Japan since 2009.
Mechanism of action:
The drug inhibits an enzyme (5-alpha-reductase isoenzymes) of type I and II, which controls the conversion of testosterone into dihydrotestosterone (DHT). The type I enzyme is found in the sebaceous glands of the face and scalp of adults, in the epidermis, sweat glands, hair follicles, hair roots of the occipital hair, liver, adrenal glands and kidneys. Several studies show that this preparation increases the diameter and number of hairs more than the drug developed in 1998 [51][52][53].
Application:
This medication is not approved for the treatment of hair loss in Germany. In South Korea and Japan, the tablets are used in a dosage of 0.5 milligrams once a day to treat hereditary hair loss.
Side effects:
The side effects of this enzyme inhibitor are similar to the side effects of the preparation approved in 1998.
Vitamins and dietary supplements against hair loss
Around one in two US citizens takes dietary supplements [54]. Around 7 billion US dollars are spent on food supplements worldwide every year [55]. Despite their great popularity, it must be noted that there are no high-quality, independent studies that prove the benefits of dietary supplements [56].
In contrast to medicinal products, proof of efficacy is not required for manufacturing and marketing. There are also no laws that protect consumers from misleading advertising promises, as is the case with prescription-only medicines. Nevertheless, food supplements are not free of side effects or interactions. Many suppliers make misleading advertising promises or misleading statements about the actual daily requirement of vitamins and trace elements [57]. Below you will find an overview of dietary supplements that are often offered to strengthen hair growth:
Vitamin A describes a group of substances that has numerous functions in the body, including the renewal of the epidermis, vision and the body’s defenses [58]. Two forms of this vitamin are ingested with food: retinol and beta-carotene. Retinol is found in dairy products and calf’s liver, for example, and beta-carotene is found in sweet potatoes and pumpkin, among other things. A vitamin A deficiency can be ruled out with a balanced diet of fruit and dairy products. The recommended daily amount of vitamin A is expressed in retinol activity equivalent (RAE), where one RAE corresponds to 1 μg of retinol. The daily requirement varies between 400 and 1300 RAE depending on age and gender. Vitamin A intoxication can occur in the long term if more than 10,000 RAE are ingested per day [59]. An overdose of vitamin A can lead to hair loss and eyelash loss [60]. Other symptoms include tiredness, malaise, weight loss, nail growth disorders and flaky skin [61]. The simultaneous administration of vitamin E increases the risk of vitamin A intoxication [62]
The vitamin B group includes diamine (B1), riboflavin (B2), niacin (B3), pantothenic acid (B5), pyridoxine (B6), biotin (B7), folic acid (B9) and cobalamin (B12). The recommended daily dose of these vitamins is achieved through a balanced diet. Vitamin B2 is a component of important enzyme accelerators: flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD) and is therefore important for energy metabolism. Vitamin B2 is found in dairy products. Vitamin B9 is important for cell division and is abundant in green leafy vegetables, citrus fruits and animal products. Vitamin B12 is needed for cell division and nerve metabolism, among other things. Vitamin B12 is found in meat, dairy products and eggs. A strict vegan diet can therefore lead to a B12 deficiency after several months [63]. The benefits of vitamin B supplements in a healthy diet have not been scientifically proven.
Vitamin C, also known as ascorbic acid, is abundant in citrus fruits, potatoes, tomatoes, green peppers and cabbage. It is an antioxidant and protects the body from damage caused by free radicals [64]. Free radicals are produced, for example, by tobacco smoking, environmental toxins and UV radiation. Vitamin C is required for the formation of collagen, L-carnithine and nerve cell messengers [65]. Vitamin is also important for iron absorption in the intestine and iron transport as well as iron storage in the body. Women should consume 75 milligrams per day and men 90 milligrams of vitamin C [66]. The body’s vitamin C stores are depleted after about three months of a very unbalanced diet. The deficiency symptom is summarized under the name scurvy. Hair loss is not one of the manifestations of vitamin C deficiency (Fleming J.D., Martin B., Card D.J., 2013, Clin Exp Dermatol.).
There are two forms of vitamin D. Vitamin D2 (ergocalciferol) is found in shiitake mushrooms and button mushrooms. Vitamin D3 (cholecalciferol) is mainly produced in the skin under the influence of sunlight (UVB radiation). Other foods rich in vitamin D3 are salmon, sardines and egg yolk. The metabolism of vitamin D2 and D3 are very similar. Vitamin D triggers the production of certain proteins in the cell nucleus. The most important sites of action include the skin, the intestines, the bones, the parathyroid gland and the immune system. The daily requirement of vitamin D is estimated at 400 to 1000 IU (international units) per day [67]. Vitamin D deficiency is widespread and affects over 60 percent of the adult population [68]. Many foods are therefore fortified with vitamin D, such as orange juice or milk (40 IU per 100 milliliters). The connection between hair loss and a vitamin D deficiency is controversially discussed [69]. If there is no vitamin D deficiency, the benefits of a dietary supplement should be critically questioned.
Vitamin E refers to a group of different substances, of which α-tocopherol is the most important representative. Like vitamin A and vitamin C, vitamin E has an antioxidant effect and thus protects against free radicals. Vitamin E is found in cooking oils, nuts, seeds and wholegrain cereals. Studies have not shown any benefit of vitamin E supplements for hair growth [70]
Iron is an important building block of every human cell and is particularly needed for oxygen transport in the bloodstream and in the muscles. Almost two thirds of the iron in the body is in the red blood cells, 25 percent is in iron stores (liver, spleen and bone marrow), and 15 percent is in muscle tissue [71]. Food sources of iron are meat, poultry and fish, as well as cereals, pulses, fruit and vegetables. The incidence of iron deficiency in men in industrialized countries such as the USA is five percent, in women 10 percent [72]. The most common cause of iron deficiency in women is heavy menstrual bleeding. The most common symptoms of iron deficiency include tiredness, muscle weakness, shortness of breath and hair loss. However, if there is no evidence of iron deficiency, supplementing with iron will not bring any benefits [73].
Zinc is an important trace element that is required by many enzymes. The Recommended Daily Allowance (RDA) of zinc is 10 milligrams (DIRECTIVE 2008/100/EC of 2008). The normal zinc level in adults is between 70 and 250 micrograms per deciliter. The trace element is mainly found in meat, fish, shellfish and poultry. The phytic acid contained in pulses, cereals and bran can inhibit the absorption of zinc. Chronic intestinal disease or a strict vegetarian diet can lead to a zinc deficiency. A deficiency is compensated for by taking zinc tablets (one milligram per kilogram of body weight per day) for one to two weeks. Supplementing with zinc is only beneficial if there is a deficiency [74].
Copper is a catalyst for many enzymes involved in cellular respiration and hormone metabolism. The Recommended Dietary Allowance (RDA) for adult men and women is 0.9 milligrams per day. In the body, copper is stored in muscle tissue and bones. A copper deficiency is rare. The causes include unbalanced artificial nutrition through infusions in seriously ill people and rare hereditary copper metabolic diseases. Copper is found in foods such as meat, seafood, nuts, seeds, wholegrain products, pulses and cocoa. In the blood, 60 to 95 percent of copper is bound to the protein ceruloplasmin. Copper deficiency is determined by determining the coeruloplasmin level (less than 20 milligrams per deciliter) and the unbound copper in the serum (less than 60 micrograms per deciliter or 10 micromoles per liter). There is no evidence that supplementing the diet with copper can stop or prevent hair loss.
Magnesium acts as a catalyst in numerous cellular respiration enzymes and in the production of genetic building blocks. In the body, magnesium is mainly stored in the bones. The most important food sources of magnesium are vegetables, fruit, cereals and nuts [75]. Magnesium blocks the transport of calcium from the muscle cells. If there is a magnesium deficiency, the calcium in the muscle cells increases. A magnesium deficiency can therefore lead to muscle cramps and high blood pressure [76]. There is no scientific evidence for the benefits of magnesium supplements for hair loss.
Selenium is important for the function of many enzymes in the body and for the immune defense. Enzymes that rely on selenium protect against free radicals, metabolize thyroid hormones and produce building blocks of genetic material, for example [77]. Selenium-rich foods include seafood, meat, cereals and grains. Brazil nuts have the highest selenium content. Both too much and too little selenium can endanger your health. Ingesting too much selenium can cause hair and nail loss, nervous system and skin disorders and paralysis [78].
Biotin is important for the function of certain enzymes and for gene regulation. Biotin-rich foods include egg yolk, calf’s liver and some vegetables. The daily requirement of biotin is estimated at 5 to 35 micrograms per day (21-143 nmol/day) [79]. A lack of biotin leads to skin rashes, inflammation of the conjunctiva, hair loss, impaired coordination and seizures. A biotin deficiency can be detected by an increased excretion of 3-hydroxyisovaleric acid in the urine [80]. Supplementing with biotin is considered safe, as excess biotin is excreted in the urine. Supplementing with biotin can falsify the test results in the event of a heart attack and thus delay timely life-saving treatment [81]. A biotin deficiency is observed when taking certain medications (carbamazepine, phenytoin and phenobarbital, isotretinoin), in older people, malnutrition, excessive alcohol consumption and tobacco smoking. Unless a deficiency has been proven, supplementing with biotin does not bring any measurable improvements in hair growth [82] [83].
Home remedies for hair loss
There are almost countless home remedies, natural remedies and shampoos available to combat hair loss. Unlike with prescription drugs, manufacturers are not obliged to provide evidence of an effect. The effects of the sleeping berry (Withania somnifera, Ashwagandha in Sanskrit), turmeric and capsaicin on hereditary hair loss have not been scientifically proven. There are also no studies that prove the benefits of pumpkin seed oil or saw palmetto for androgenetic alopecia [58]. There is no scientific evidence for the hair growth-promoting effect of Schüssler salts and fenugreek. The reports on the positive effects of horsetails (Equisetum) and the dietary supplement dimethylsulfone (methylsulfonylmethane) on hair growth are not free of conflicts of interest. The studies were carried out by employees of the companies that produce and market these foods or were financed by these companies [59] [60] [61].
Our experience report on hair loss treatment
Numerous patients who suffer from hair loss and want a full head of hair again have already taken advantage of the various treatment methods at CenterPlast and shared their experiences. You can find patient testimonials and reviews in the well-known online portals for rating doctors. You will also find a separate category on this topic on our website. In addition, several patients who have undergone treatments at CenterPlast have agreed to tell interested parties about their experiences. Feel free to talk to us about this option during your personal consultation.
Our before and after pictures for hair loss treatment
It is not permitted by law to publish before and after photos of hair loss treatments on the Internet. However, you are welcome to view such images during the consultation to get an impression of the expected result.
Frequently asked questions
Treatment of hair loss should start with avoiding harmful effects on hair growth. The most important measures include
- Stop smoking cigarettes. Smokers have demonstrably thinner hair than non-smokers [62]. Smoking reduces blood flow to the hair root, damages the genetic material of the hair root, promotes the release of inflammation-promoting messenger substances and changes the hormone balance [63].
- Regular exercise is good for your health and prevents hair loss [64]. There are several possible explanations for this. On the one hand, toxins and waste products are excreted through sweating [65]. Exercise, on the other hand, promotes stress reduction and increases blood flow to the skin. Exercise regulates hormone levels, improves sugar metabolism and blood pressure [66].
- Eat raw vegetables (lettuce, raw carrots and tomatoes) and fresh herbs (rosemary, sage, parsley, basil) at least three times a week. Mediterranean cuisine protects against hair loss [67]. The observation is explained by the antioxidant and anti-inflammatory effect of secondary plant substances. The numerous indications of the health-promoting influence of Mediterranean cuisine underline this observation [68].
- Pay attention to your body weight. Being overweight leads to thinner hair. This can be explained by the fact that a high-fat diet leads to the release of inflammatory signals in the stem cells of the hair roots [69].
- Avoid stress and make sure you get enough sleep. A part of the diencephalon (hypothalamus) releases an increased amount of a certain hormone (corticotropin-releasing hormone) during stress. This hormone causes the release of histamine from defense cells at the base of the hair follicles. Histamine finally initiates the regression phase (catagen phase) of the hair follicles [70].
- Protect your hair from excessive sunlight. Sunlight (UV-A radiation) causes a decline in stem cells and pigment cells in the hair roots [71]. Certain degradation products of normal skin germs (propionibacteria) can be harmful to cells when exposed to sunlight (light-activated porphyrin) [72]. Free radicals generated by the sun lead to a reduction in hair pigment. Lighter hair offers less protection from UV light [73].
- Take targeted action against dandruff. Various microorganisms colonize the scalp and form a natural protective shield (propionibacteria, Staphylococcus bacteria and Malassezia yeasts). The yeast fungus Malassezia accounts for 45 percent of skin germs in healthy people. If you have oily skin, the yeast can multiply more, trigger an inflammatory reaction and promote hair loss [74]. In people with dandruff, the proportion of yeast in the skin flora increases to 75 percent [75]. The yeast fungus Malassezia is involved in seborrhoeic dermatitis, psoriasis and atopic dermatitis. Shampoos with the active ingredients zinc pyrithione (for example Head & Shoulders®), ciclopirox olamine (for example Stieproxal®) or ketoconazole (for example Ketozolin®) reduce Malassezia colonization [76].
As a rule, health insurance companies do not cover the costs of hair loss treatments. There are two reasons for this:
- Your health insurance will pay for services that are urgently required for medical reasons.
- A recommendation from the Federal Joint Committee (G-BA) must be available for the costs to be covered.
Muscle relaxants are offered for the treatment of congenital hair loss under the idea that relaxing the scalp muscles improves blood flow and oxygen supply to the tissue. However, there are no reliable studies that prove the effect of muscle relaxation [77].
Around five to ten percent of the hair on the scalp is in the resting phase (telogen phase). At this stage of the hair cycle, hair falls out over a period of four months. Around 80 hairs are lost every day, usually with every hair wash [78]. Hair loss, also known as effluvium, means that more hair falls out than grows back. Hair loss can be described or categorized according to several aspects:
- The cause: hormones, inflammation or injury to the hair root can lead to hair loss.
- Duration: Hair loss can occur gradually over years (chronic) or suddenly over a few weeks (acute). If it lasts for more than six months, it is referred to as chronic hair loss.
- The affected region: Hair loss can affect the entire scalp (alopecia totalis), the entire body (alopecia universalis) or only localized areas.
- The affected hair cycle: If the hair is damaged during the growth phase, for example by chemotherapy, radiotherapy or repeated plucking, this is referred to as anagen effluvium. If you notice a lot of hair falling out – in other words, if many hairs enter the resting phase at the same time, for example due to extreme dieting (crash diets) or emotional stress, this is known as telogen effluvium.
- The recovery of the hair follicles: A distinction is made between non-cicatricial and cicatricial hair loss (cicatricial alopecia). Scarring alopecia results in permanent damage to the hair follicles, for example as a result of severe inflammation or a burn. As a result, hair no longer grows back in the affected area.
The most common forms of hair loss are congenital hair loss (androgenetic hair loss), followed by circular hair loss (alopecia areata) and diffuse hair loss (telogen effluvium). Rare forms of hair loss include hair loss caused by pressure or traction (traumatic alopecia) and fungal disease of the scalp (tinea capitis).
The most frequently discussed causes include
- Hereditary hair loss due to male hormones (androgenetic alopecia)
- Hormone fluctuations due to pregnancy, childbirth or the menopause
- Hyperthyroidism or hypothyroidism
- Stress [79]
- Overweight [80]
- Extreme diets [81]
- Cigarette smoking [82]
- Lack of vitamins and trace elements (detailed information on the respective food supplements can be found enclosed)
- Air or water pollution (further information can be found on this page)
- Harmful hair care products
- Certain hairstyles (boxer braids, rasta braids)
- Serious life-threatening illnesses [83]
- Severe dysfunction of the liver or kidneys
- Various medications (detailed information is enclosed)
For some influences, the cause-and-effect relationship has not been proven beyond doubt. The multitude of causes discussed and the delay with which hair loss occurs make scientific proof difficult. You can find out more about this in our encyclopedia of cosmetic surgery under the entry Cause.
In the vast majority of cases of hair loss, the type of hair loss can be determined during a consultation and physical examination. In cases of doubt, the following further examinations can be arranged.
Pluck test:
The pull test involves carefully checking how firmly the hair is anchored at various points on the scalp. The test is considered positive if more than ten percent of the hair comes loose under light tension. A positive test means that the hair follicles have entered the resting phase (telogen phase) prematurely (telogen effluvium). However, the test can only be evaluated if you have not washed your hair for at least 24 hours beforehand.
Blood test:
Special examinations of a blood sample provide indications of diseases that can cause hair loss. An iron deficiency is determined by examining the red blood cells, the amount of oxygen-transporting hemoglobin and the amount of iron-storing ferritin. Thyroid hormones are determined if a disease of the thyroid gland is suspected. If there is reason to suspect a disorder of the sex hormones, the male hormone testosterone and the hormones of the pituitary gland, the luteinizing hormone and the follicle-stimulating hormone are determined. If there are indications that a sexually transmitted disease (syphilis/lues) has caused the hair loss, a test for antibodies will be arranged. In the case of unexplained hair loss in unusual places, further specific tests, such as the detection of pollutants, can be requested.
Pathogen detection:
The appearance of circular redness, crusts, scales and brittle hair, especially in children, can be a sign of a fungal infection. If a fungal infestation of the scalp is suspected (tinea capitis), samples of skin flakes or hair are examined under the microscope for traces of fungus. Differentiation from other skin diseases (psoriasis, seborrheic and atopic eczema) should be made by a dermatologist.
Standard photo documentation of the scalp overview:
The aim of the documentation is to record the initial condition of the scalp hair and the success of the treatment. The paired comparison of before and after photos provides information about the hair density and changes in the hairline. For a meaningful comparison, a uniform and repeatable position of the head, camera setting and exposure must be observed. A change in hairstyle or hair color complicates the comparison. The four common images include the tonsure (vertex), the middle parting, the hairline above the forehead (forehead-hairline) and the hairline above the temples (receding hairline). The initial condition and the findings are usually photographed after three, six and 12 months.
Examination of epilated hair under the microscope (trichogram):
This method is used to determine the hair diameter and growth behavior (anagen/telogen ratio) of 60 to 80 scalp hairs. Depilation of scalp hair for examination purposes is hardly ever used any more. There are several reasons for this: the epilation process can cause hair damage and is painful. Thin downy hairs and short hairs cannot be examined using this method. Other examination methods (TrichoScan®) are simpler, faster and more accurate.
Computer-aided examination of growth behavior (TrichoScan®):
The examination is carried out using a high magnification camera (20x magnification) and automatic image analysis. The TrichoScan® examination is quick and uncomplicated. However, the accuracy and susceptibility to errors of the software are critically discussed in scientific publications [84]. For the examination, an area of one square centimeter on the scalp is marked and shaved. To improve the reliability of the automatic image analysis, the hair is dyed dark and photographed after 48 to 72 hours. The examination is used to evaluate treatment methods, usually as part of clinical studies. The following parameters are determined with the TrichoScan®:
- the hair density (number of hairs per square centimeter, standard value for Europeans: 220 hairs per square centimeter),
- the thickness of the hair (micrometers, standard value for Europeans approx. 65 micrometers),
- the growth rate (millimeters per day, standard value 0.3 millimeters per day),
- the number of downy hairs (hairs with a diameter of less than 30 micrometers, ratio of normal hairs to vellus hairs normally 7:1),
- the growth phases (cycles) of the hair follicles (anagen-telogen ratio: 9:1).
Tissue sample of the scalp (biopsy):
The tissue sample is primarily used to assess the hair follicles but also the sebaceous glands. Under the microscope, a distinction can be made between scarring and non-scarring hair loss. Under local anesthesia, four millimeter samples of the scalp are punched out. In order to capture the hair follicles, the sample must have a layer thickness of at least four millimeters. Normally 35 to 40 hair follicles are recorded in one sample. The tissue is examined in several layers. The preparation and analysis of the tissue samples requires a great deal of experience and is time-consuming. The following variables can be determined in a tissue sample:
- the number of hairs,
- the thickness of the hair (micrometers, standard value for Europeans approx. 65 micrometers),
- the growth phases (cycles) of the hair follicles (anagen-telogen ratio: 9:1).
- the number of downy hairs (hairs with a diameter of less than 30 micrometers, ratio of normal hairs to vellus hairs normally 7:1),
- Signs of inflammation of the hair follicles.
Hair analysis (hair mineral analysis):
Hair analysis is generally used for criminal investigations (forensic examinations), the detection of poisoning or the detection of doping substances. Examinations of the blood or urine provide information about short-term current changes in the metabolism. The hair analysis allows conclusions to be drawn about changes that took place weeks or months ago. Foreign substances only accumulate in the hair after a longer period of time. The detection limits vary depending on the substance and hair metabolism. For naturally occurring substances (e.g. trace elements), the standard values (reference ranges) vary greatly [85]. It is therefore difficult to interpret the concentrations of naturally occurring substances. The detectable substances include
- Pollutants (nicotine, mercury, arsenic, lead)
- Narcotics (cannabionoids, cocaine, amphetamines)
- doping agents (male sex hormone testosterone, nandrolone).
During the consultation (anamnesis), information is collected about the type of hair loss and the possible causes. Fri. Dr. Santos Stahl will therefore ask you a few questions, such as:
- When did the hair loss first occur?
- What food do you eat?
- How often do you wash your hair and with which products?
- Do family members suffer from hair loss?
- Are you exposed to particularly stressful situations?
- Are you taking medication or dietary supplements? Do you smoke?
The areas affected by hair loss are then examined. The hair color, hair density and hair thickness are examined with a magnifying glass. The scalp is examined for dandruff, redness and scars. Fri. Dr. Santos Stahl examines the tensile strength of the hair and the strength of the nails. In case of doubt, further examinations are arranged to clarify the causes of hair loss. Finally, a treatment plan is drawn up. The scalp is photographed to assess the development. The chances of success and the costs of various treatment options (finasteride, minoxidil, therapy with the body’s own blood, microneedling, injections with muscle relaxants) will be discussed with you. You are welcome to make an appointment for hair loss treatment after the consultation.
The hair follicle goes through regular cycles of growth, regression and rest in the course of life. In each cycle, a new hair is formed and the old hair is shed. The hair cycle consists of the following three phases:
- Growth phase (anagen phase): The phase begins with cells that multiply in the area of the hair root to form a cell cluster (dermal papilla). Specialized horn-forming cells (keratinocytes) develop from the stem cells. The further developing horn-forming cells produce a new hair. A new hair root sheath also forms around the new hair. The old hair is displaced by the new hair that grows back until it finally falls off. The new hair grows for two to seven years at a rate of around one centimeter per month, depending on the individual and age.
- Regression phase (catagen phase): The phase begins with the detachment of the cell cluster (dermal papilla) below the hair bulb (bulbus). The hair becomes detached from its blood supply. The cells in the lower two thirds of the hair follicle undergo a scheduled programmed cell death. The hair bulb and the inner part of the hair root sheath recede. The cell formations move to more superficial layers of the skin. The recovery phase usually lasts about two weeks. During this time, the old hair remains in the canal through which the new hair will emerge.
- Resting phase (telogen phase): In this phase, the hair falls out (medical term effluvium). The renewing cell cluster (dermal papilla) and the hair bulb (bulb) approach each other. Stem cells are activated and a new cycle is initiated. With each subsequent cycle, the duration of the resting phase increases, which slows down hair renewal overall. The resting phase lasts up to four months.
At any given time, around 90 percent of the hair is in the growth phase (anagen phase), one to three percent in the regression phase (catagen phase) and five to ten percent in the resting phase (telogen phase). When determining the anagen-telogen ratio, the hairs in the catagen phase are added to the hairs in the telogen phase.
- Washing your hair too often leads to hair loss.
There is no scientific evidence to support this statement. However, there is a lot to consider when choosing the right shampoo. - Frequent cutting makes your hair grow faster.
Cutting the ends of the hair removes split ends. High temperatures when blow-drying or using a curling iron as well as chemical hair straightening can lead to brittle hair shafts and split ends. Hair growth takes place in the hair roots and is not affected by cutting the ends of the hair. - Frequent hair washing causes greasy hair.
Fats are produced in the sebaceous glands of the hair and secreted onto the surface of the skin. The production of sebum by the glands is controlled by hormones, among other things. A tendency to dry or oily skin is often genetically predisposed. Washing the hair removes dandruff and oil from the scalp, which protects the skin pores from clogging and thus from inflammation. Sebum production is neither increased nor reduced by washing the hair. - Frequent brushing stimulates blood circulation to the scalp and promotes hair growth.
There is no evidence for this assertion. Brushing or combing too quickly can lead to knots in the hair. Combing too hard can cause the hair to pull out or damage the hair shaft. Straight European hair is fluffy when dry. Wet hair takes on a compact shape, with the individual hairs sticking together strongly over large parts of their length. Disentangling by the moving comb is difficult due to the low stiffness of the fibers. The increased friction between the fibers and the comb makes combing even more difficult. Unlike straight European hair, which is more difficult to comb wet than dry, wet combing African hair is easier than dry combing [86]. - Caffeine shampoos make hair grow back.
There is no evidence that shampoos containing caffeine have a growth-promoting effect. The dilution with water and the short exposure time during hair washing underline the doubts about the advertising promises. - Chemical straightening or heat cause hair loss.
The extent of the damage depends on the type and frequency of hair treatment. Sensitivity also depends on age and hair type. The use of chemical hair straighteners can cause frizzy hair, dandruff, hair loss, gray hair, hair breakage and split ends [87]. - Men prefer women with longer hair.
According to studies, women with long hair are seen as more feminine, younger, healthier and more attractive than women with short or pinned-up hairstyles [88]. Another study comes to the conclusion that men rate women with long hair as more feminine, determined, intelligent, independent and healthy. Women with short hair were perceived as more honest, caring and emotional [89]. There is another study result that we would like to share with you:
Women’s hairstyles have an influence on men’s willingness to help. A woman who drops a glove on the ground in a pedestrian zone is more likely to have it picked up by male passers-by if she wears her hair down than if she ties it up in a pony or bun [90]. - Men prefer blonde women.
Several studies reported that men, but not women, rated a woman with blonde hair as more attractive [91] [92]. Other studies have found that drivers are more likely to think blonde women are hitchhikers than dark-haired women [93]and that blonde waitresses get more tips than dark-haired ones [94].
Medication can cause hair loss. With many drug treatments, the mechanism that leads to hair loss is not yet understood. In order to avoid liability for breach of the duty to provide information in accordance with Section 84 AMG, pharmaceutical manufacturers list all even remotely possible and unspecific side effects. This is why “hair loss” is listed as a possible side effect on many package inserts. The more common relevant medications include heparin injections and the pill. Hair loss is often noticeable two to four months after the start of treatment. Below you will find some examples of active ingredients for which increased hair loss has been observed.
| Areas of application of the active ingredients | Active ingredient |
| Attention deficit disorder | Amphetamines |
| Treatment of malaria | Chloroquine |
| High blood pressure | Propranolol (beta-blocker) |
| High blood pressure | Metoprolol (beta-blocker) |
| High blood pressure | Captopril |
| High blood pressure | Enalapril |
| Blood thinning | Heparin |
| Blood thinning | Phenprocoumon |
| Breast cancer | Tamoxifen |
| Depression | Lithium |
| Depression | Fluoxetine |
| Epilepsy | Phenytoin |
| Gout | Allopurinol |
| Gout | Colchicine |
| Cardiac arrhythmia | Amiodorone |
| HIV | Indinavir |
| Hormonal contraceptive | Pill |
| Cancer | Cyclophosphamide |
| Cancer | Doxorubicin |
| Parkinson’s disease | Levadopa |
| Rheumatism | Sulfasalazine |
| Rheumatism | Penicillamine |
| Rheumatism | Gold |
| Hyperthyroidism | Carbimazole |
| Hyperthyroidism | Propylthiouracil |
| Hypothyroidism | L-thyroxine |
| Schizophrenia | Risperidone |
| Testosterone deficiency | Testosterone |
| Suppression of the body’s defenses | Tacrolimus |
| Suppression of the body’s defenses | Azathioprine |
| Suppression of the body’s defenses | Methotrexate |
| Viruses, cancer or autoimmune diseases | Interferons |
| Vitamin A deficiency | Retinol |
| Vitamin E deficiency | Tocopherol |
| Prevention of malaria | Proguanil |
| Water retention | Spironolactone |
| Diabetes | Glibenclamide |
Sources: Sinclair R., 1999, International Journal of Dermatology and Piraccini B.M., Iorizzo M., et al, Current Drug Safety, 2006.
Even with a mild course, a COVID-19 infection is associated with considerable stress, usually due to reduced social contacts. It is assumed that stress can trigger acute diffuse hair loss [95]. In principle, however, medication taken during an infection can also trigger hair loss. On average, ten percent of COVID-19 infected patients exhibit diffuse hair loss. Hair loss occurs 50 to 60 days after a positive COVID-19 test. Possible treatments include minoxidil solution and injections of the patient’s own blood [96].

AUTHOR
Dr. Adelana Santos Stahl
Our aim is to offer optimal, discreet and precise treatment based on our extensive expertise in the field of plastic surgery.
Dr. Adelana Santos Stahl has a unique international perspective with a female view of plastic surgery. Your individual and detailed approach is the key to the beautiful and natural results. Having trained in Brazil, one of the largest and best-known countries for aesthetic and reconstructive plastic surgery, she understands her patients’ desire to look and feel their best.
She completed her medical studies and training as a specialist in plastic and aesthetic surgery in Brazil. In 2009, she also successfully passed the German equivalence examinations for the state medical examination.
Two years later, in 2011, she received the German and in 2012 the EU specialist certification (EBOPRAS) for plastic surgery. From 2009 to 2013, she deepened her knowledge of aesthetic and reconstructive facial surgery with world-renowned representatives of plastic surgery such as Professor Gubisch at the Marienhospital and Madame Firmin in Paris.
A VDÄPC Fellowship (continuing scholarship for graduate students) in Switzerland, France and the USA has further enriched her professional experience. Dr. Santos Stahl is active in various renowned professional associations. In addition to the DGPRÄC and DGBT, she is also a member of the Brazilian Society of Plastic Surgery – SBCP.
She is also the author of several scientific articles and, together with her husband, is dedicated to research and clinical studies in the field of plastic surgery.
She has been based in Saarbrücken since 2019.
You might also be interested in




Personal advice
We take time for you and offer you customized advice and treatment for your individual result.



